
The Pandemic, lockdown, and the chain of events that followed made the country wake up to the state of the most unfortunate group of the labour force; the migrant workers. They have always remained invisible to the development agenda of the government and only the catastrophe of a pandemic could shed light on their woes. Among this invisible workforce, there remains yet another marginalised group of female migrants.
In India, female migration was initially considered insignificant by equating their movement merely as associational or followers of men. However, this has certainly changed in the last decade. Marriage was seen as the central motive behind female migration, though lately more women are seen to enter the labour market post-migration as their labour demand rose in sectors of so-called “female occupations” of domestic work, care-work and certain informal labour requirements in sectors such as in construction, garment work, food services and as coolies and vendors. As family migration from rural to urban abodes saw a rise in the country, both male and female migrants were required to join the labour force to meet their mere subsistence needs. Lack of employment, low income and other economic reasons pushed females, especially from rural areas, to migrate to urban zones of the country (Singh et al., 2015). While in urban areas, the migrants especially females and children are exposed to extreme vulnerabilities with regard to their dismal conditions of work in the informal sector, urban policies are deeply flawed in omitting migrant welfare and the sheer denial of their civil rights and entitlements.
Precarious domestic work and female migrants
Domestic work is often regarded as an invisible and insignificant addition to the social and economic values of a country. The work is increasingly feminised with over 80% of the world’s domestic work occupied by women (International Labour Organisation [ILO], 2013a). And this mirrors the traditional notions of domestic work being a woman’s task. These tasks include traditional housework such as cleaning, cooking, washing clothes or utensils etc. or care-work such as a child or elderly care. Female migrants with low skills, low levels of education and migrating from rural abodes in search of employment form a predominant part of the labour pool. With no recognition and regulation of work, the female domestic workers are subject to unequal power dynamics at the workplace, making their lives precarious in terms of wages, security and wellbeing.
In India, domestic work employment among females saw an upsurge, especially in urban areas. This surge is mainly accounted for by the increasing need for care work given the changing demography, lack of work opportunities in other sectors and the gender constructions moulded by the society (Chandrashekar & Ghosh, 2012). According to the National Sample Survey (NSSO-2011-2012, 68th round), 39 lakh (3.9 million) people are occupied in domestic work, among which 26 lakh (2.6 million) are females. Micro-level surveys suggest a predominant concentration of female migrants in domestic work, especially in urban areas (Mazumdar et al., 2013). There are two forms of workers: live-in workers, who are accommodated in the household and live-out workers, who return to their respective houses after work and may be involved in work with multiple households. As there is no relevant national data on migrant workers involved in the sector, micro-level surveys or sector-based studies are the only sources in understanding the conditions of these migrants in domestic work. Studies have stated that migrants with low vocational qualifications and often seen as unregulated and undocumented cheap labour, work under low wages for long hours and in dismal working conditions affecting their health and safety. Live-in domestic workers are more prone to the dangers of sexual and physical abuse. Live-out domestic workers migrating to a new city, struggle with the inaccessibility of social security schemes and entitlements. Exploitation by private placement agencies in terms of wages and work conditions is another area among their hassles.
The domestic work arena, already an unregulated and unorganised sector, puts female migrants with low bargaining power on a higher vulnerability scale. The task of identifying domestic work hinders the formulation of a sound regulatory mechanism to confront such vulnerabilities.
Barriers to effective Regulation
Regulating domestic work is impeded by cultural and structural barriers. The traditional notion and disregard of domestic work by women in households is extended to the understanding of paid domestic work as unproductive and hence, making it undervalued. The structural barriers relate to the unusual workplace in private spheres, which makes it difficult in enforcing labour laws and any form of scrutiny against the privacy norms of a household. The informality of work and its complexities aggravates the barriers in regulation. The employment relationship is uncertain as it is without any legal titles of employee and employer, making the relation very personalised and often not under any form of contract or agreement. Even if labour laws are made inclusive of domestic work, implementation and assurance of compliance of these laws in households are challenged until the household is recognised as a ‘workplace’ and the person hiring as an ‘employer’ in the legal framework (Chen, 2011).
Even though these barriers existed, the International Labour Organisation (ILO) convention 2011 attempted in ensuring decent work to domestic workers and this is recognised as the most important landmark in identifying domestic work under a legal framework. ILO defines domestic work as “work performed in or for a household or households” and domestic worker as “any person engaged in a domestic work within an employment relationship”. The convention specified a comprehensive labour standard for domestic workers in areas of their wages, hours of work, occupational safety and health and social security. The convention addressed and standardized the various concerns in the sector regarding child labour, migrant workers, trafficking, live-in domestic labourers and private recruitment agencies (C189 – Domestic Workers Convention, 2011). Even after the completion of 10 years of the convention and 32 ILO member countries enforcing the landmark treaty, India is yet to ratify the convention.
As domestic work remains undefined in the country, no significant statistical standard in estimating domestic workers exist. In the ILO policy brief on “Global and regional estimates of domestic workers” (ILO, 2013b), ambiguous nature of data on domestic workers were noticeable from the widely distributed figures, ranging from 2.5 million estimates from a household survey, 4.5 million workers estimated from official statistics (NSSO 2004-05) to an exaggerated figure of 90 million in news media. This difference in estimation is related to the difference in the identification of domestic work among different establishments (Mahanta & Gupta, 2015). With no clarity in identifying domestic workers inclusive of its peculiarities, these figures could be heavily underestimated too. Being a female migrant in the sector aggravates the problem of estimation as National statistics narrows down female migration patterns merely as associational. And thus failing to understand the true motives behind female migration and the subsequent scale of occupations they reside in (Indu et al, 2012). Macro data narrows down domestic female labour into regular workers based on their duration in employment and disregarding the conditions of low wages and other insecurities, while the temporary and casual nature of work goes unrecognised (Neetha & Indrani, 2020). The informality of work is another area that India has failed to regulate. Labour laws for industrial labour often disregard informal workers. This is evident in the isolation of migrant workers, especially female migrants in domestic work (Poddar & Koshy, 2019).
Lacunae in the legal framework
Domestic work and most feminised occupations, in general, in unorganised sectors, are isolated from the legal framework given their unique characterisation of workplace and employment relationships and not to mention the challenges in recognising their work given the cultural and structural barriers. For female migrants in domestic work or any other informal activity, the situation is similar.
There were certain positive steps in attempting to recognise the domestic workforce in the country. First of such attempts were their inclusion in the Unorganised Workers Social Security Act 2008 which gave hope, but failed to be implemented across different states (Agrawal & Agarwal,2018). Subsequently, the government also set up a task force to recommend a framework for policymaking and after 10 years, in 2019, we see a draft on National policy on domestic work formulated by the government covering their recognition, access to civil rights and social security schemes, skill development, regulating private placement agencies and a grievance redressal system (“National Policy for Domestic Workers”, 2019). Upon the recommendations of the task force, the domestic workers were to be included under the National Health insurance scheme – Rashtriya Bhima Yojana (RSBY). But the limited awareness of the scheme, its functioning and benefits, coupled with corruption reduced the domestic worker’s accessibility of the same (Mahanta & Gupta, 2015). The suggestion of the task force to include domestic worker rights in existing legislations, pertaining to industrial or organised labourers, was widely criticised because it does not adapt to the peculiarities of the feminised domestic work (Poddar & Koshy, 2019). Ensuring minimum wages to the domestic worker through the Minimum Wages Act 1948 with a task-based approach, while ignoring the aspect of personalised nature of employment completely, puts the live-in workers whose tasks are not quantifiable, out of the ambit of the act’s provisions. Similarly, the inclusion of domestic workers in the Sexual Harassment of Women at Workplace Act (2013), Employees’ State Insurance Act (1948) and Unorganized Workers’ Social Security Act 2008 is considered inadequate. Even though such inclusion is appreciated, these legislations fail to cater to the rights of a domestic worker if they are based on organised sector labour standards and without understanding the complexities of the domestic work (Poddar & Koshy, 2019).
Private placement agencies, one of the main recruitment channels of domestic work, remain unregulated. This has led to the rise in exploitation in terms of payment and working conditions. The Delhi government drafted a Delhi Private Placement Agencies (Regulation) Bill in 2012 which was widely rejected by the domestic workers’ unions and groups. The proposed bill was criticised to be ineffective as it does not include the registration of the employers and lacks clarity in the process of inspection of these agencies (Chigateri et al., 2016). A study on one of the frequently travelled migrant routes, which is from Jharkhand to Delhi, reveals that migrants were subjected to conditions of exploitation and forced labour under such placement agencies. Conditions of forced labour are witnessed mainly among live-in domestic workers, who have to work under the agent for the stipulated period. The Inter-State Migrant Workmen’s (Regulation of Employment and Conditions of Service) Act 1978 fails to address this issue as placement agencies relating to domestic work do not come under the ambit of the act. The act considers only those labour contractors who are registered at the origin state. Placement agencies involved in domestic work function through several sub-agents and mostly are unregistered (ILO, 2015)
There were some positive responses from state governments. The state of Tamil Nadu set up the Tamil Nadu domestic workers welfare board. Similarly, Maharashtra set up a domestic worker welfare board under Maharashtra Act (Agrawal & Agarwal, 2018) in 2008 while Kerala adopted a domestic worker bill in 2009. States like Kerala, Karnataka, Andhra Pradesh, Maharashtra, Tamil Nadu, Bihar and Rajasthan have set the minimum wage rate (Madhav, 2010). Neetha and Palriwala (2011) analysed the state legal framework on domestic workers and pointed out the same inadequacies noted over and over again, that is of not recognising the intricacies of domestic work, workplace, its several sub-categories, unregulated placement agencies and its unique employment relation. With no data on domestic workers and at the same time their numbers continuing to increase, these loose legislations and provisions go unnoticed by the workers.
In 2019, with the view to improving compliance and bringing about uniformity of laws, 29 labour laws were consolidated into 4 labour codes: a) code on wages, b) code on industrial relation c) code on social security and d) code on occupational health and working conditions (“Overview of Labour Law Reforms”, n.d.). While the notion was to make the labour laws more transparent and such consolidation was expected to increase the coverage of different workers under the law, these codes remain ambiguous when it comes to certain sectors of informal work. Neetha and Indrani (2020) analyse these codes through a gender lens focusing on domestic and migrant workers. Code on wages does not incorporate private households as an entity hiring employees and thus domestic workers who struggled to attain minimum wages under the previous Minimum wages act (1948) have no mention, leaving them ambiguous. Code on industrial relations dealing with collective bargaining and industrial disputes, do not mention freedom of association in unorganised sectors and curbs the right to strike which has serious implications of registration of domestic workers under trade unions and their right to collective bargaining. Code on social security (CSS) has consolidated the unorganised workers’ social security act 2008, which was the first attempt towards the recognition of domestic workers and the new code puts the functioning of such acts and provisions for the unorganised sector under the discretion of the government, leaving out legislative scrutiny. Hence, there is uncertainty of the efficient functioning of these acts under CSS. Under the code, maternity benefits were applied only to the registered establishment of work. And domestic workers with no recognition of the workplace become ineligible for the same. Code on occupational health and working conditions is also seen to have not recognised the need for laws based on different sectors of work. It has again failed to include private households as a workplace, leaving the conditions of domestic work unregulated. Another failure relates to ignoring the Sexual Harassment of Women at Workplace Act (Prevention, Prohibition and Redressal) 2013, which further leaves out the scrutiny of abuse or exploitation of domestic workers. The fact of being migrants among domestic workers isolates them even further from these labour codes.
The lacunae in existing legislation in recognising domestic work and migrant labour continues to be beset in ambiguities with the new labour reforms.
Present scenario: Covid-19 adding to the vulnerabilities
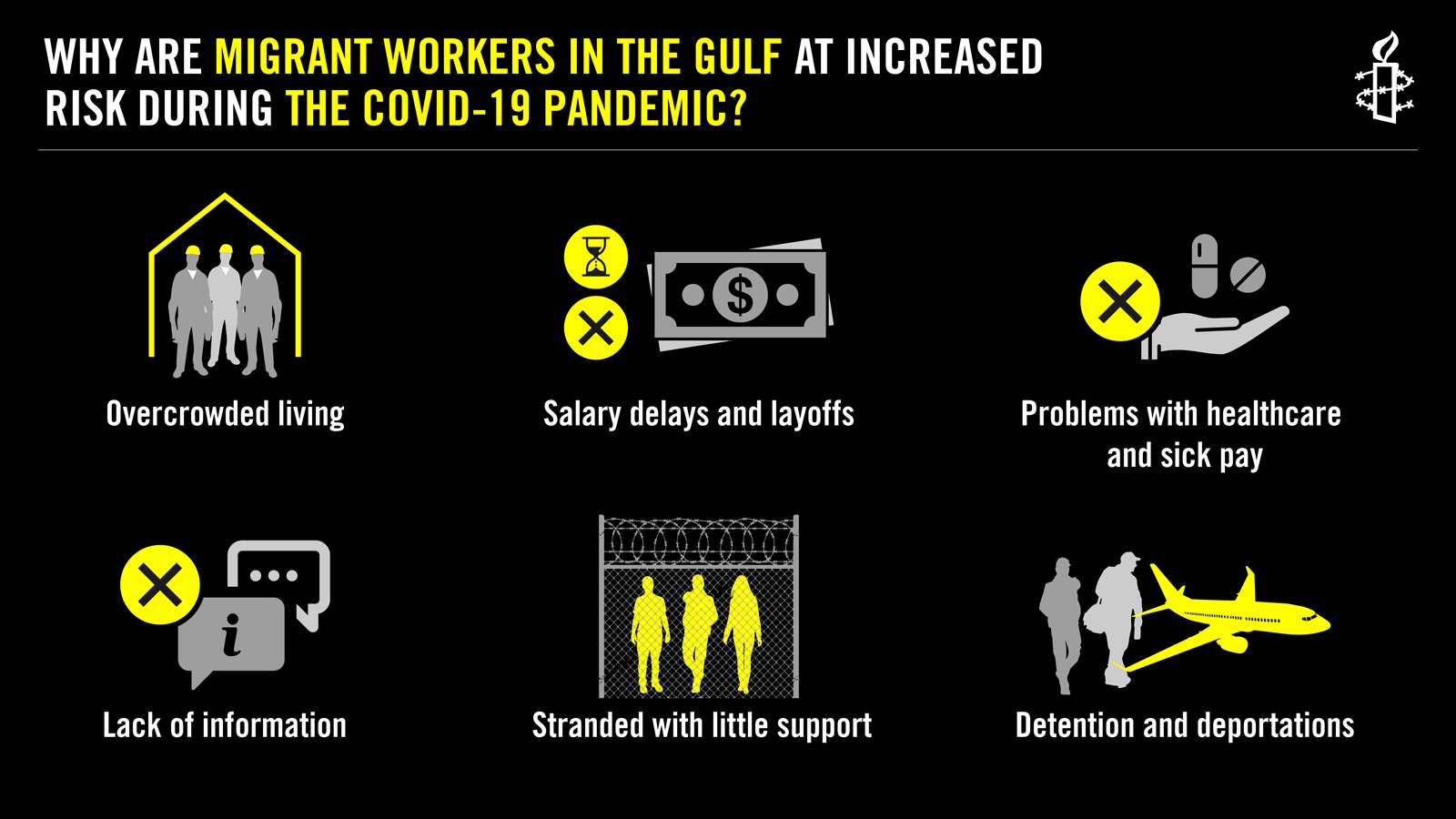
The onset of the Covid-19 and the resultant lockdowns have led to massive disruptions of normal life resulting in the shocks of sudden unemployment, financial strain and increased burden for workers in the unorganised sector. The migrant workers bore the highest brunt. In such a scenario, female migrants in an unregulated and isolated sphere of work such as domestic workers have been subject to severe distress. The lockdown and reduced mobility left the workers unemployed and without income. Live-in migrants faced increased workload but no change in wages. Even with the slow revival of the economy, they are under threat of being infected or being carriers, given their precarious work and living conditions. Sudden dismissals and financial strain have forced many to the situation of borrowing money for subsistence and eventually ending up in debt. Workers struggle to meet the basic needs of health, food, education of the family with lower income and savings (Sumalatha et al., 2021). With dismal employment relations and working conditions, coupled with the exclusion from the legal framework and social protection, Covid-19 has expanded the existing inequalities.
Government intervention: The need of the hour
Government intervention both in ensuring basic rights and providing for the welfare of the domestic workers have been negligible. The cultural and structural barriers are not the only challenges in regulating domestic work. There is a lack of political will in acknowledging domestic workers and their woes. As they remain scattered and invisible, the domestic workers are not seen as potential vote banks and hence remain without any political influence. The sector which is comprised largely of female migrants is devoid of any political voice and agency in their origin or host states since there are barriers in pursuing their voting rights given the nature of their migration. Their interactions with civic authorities and politicians in the host state are marginal and hence, their issues do not come to the fore (Bureau, 2018). There is a lack of awareness among the migrant workers on their voting rights. They are largely unaware as to who should be approached in the host state to resolve their problems. Even a migrant worker, well aware of his/her political rights and agencies, refrain from pursuing any form of interaction as they have either lost faith in the system or are disillusioned by the long time and effort spent pursuing the cases with no results to show. This highlights the need for effective political inclusion of migrant workers and the generation of political and electoral awareness among them (Bureau, 2018).
Further, identification and protection are the two essentials in creating an inclusive environment for female migrants in domestic work. The feminized nature of domestic work in the country, concentrated predominantly among poor and marginalised migrant workers, need to be recognised as dignified “work” and households they work in as “workplace”. Only separate comprehensive legislation on domestic work can incorporate the varied complexities of the sector, rather than a mere extension of organised sector legislations. Such separate legislation would provide the domestic worker with an identity that can ensure them their rights and entitlements (Sharma & Kunduri, 2015). The legislation should address the working conditions, violations and exploitations, provisions for mobilisation, illegal channels of private placement agencies and establishing basic civil rights from a gender perspective to incorporate the differential experience of females in the sector. Efficient implementation and scrutiny of the same require statistically significant data, the absence of which is another flaw in the system.
Domestic worker’s inaccessibility of social protection is the result of the lack of recognition. Migrant workers in the sector without any identity proof or formal registration are excluded from social protection schemes. Agrawal and Agarwal (2018) suggest setting up an independent welfare board in every district responsible for registering, ensuring availability of social security benefits, conducting dispute resolution, dissemination of information and providing skill development and training for domestic workers. The provision of financial incentives can help in coping with sudden unemployment situations during any form of crisis such as the pandemic. Allowing for the organisation of domestic workers into unions and cooperatives can also be beneficial in attaining social and legal protection. Domestic worker groups such as SEWA and National Domestic Workers Movement (NDWM) in the country have been attending to the woes of the domestic workers by providing a platform for collective bargaining and assertion of rights.
The introduction of the draft on National Policy on Domestic workers can be seen as a positive development, however, the policy still remains in consideration. Vulnerabilities of the domestic workers, exacerbated by the pandemic, highlight the urgent necessity for the ratification of the ILO convention on domestic workers. There is an urgent requirement in increasing the government’s sensitivity towards domestic workers and their precarious existence.
References
- Agrawal, U., & Agarwal, S. (2018). Social Security for Domestic Workers in India. Socio-Legal Rev., 14, 30
- Bureau, A. (2018). Political Inclusion of Seasonal Migrant Workers in India: Perceptions, Realities and Challenges.
- C189 – Domestic Workers Convention, 2011 (No. 189). (n.d.). Retrieved July 15, 2021, from https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C189
- Chandrasekhar, C. P., & Ghosh, J. (2012, November 12). Changing patterns of domestic work. @businessline. https://www.thehindubusinessline.com/opinion/columns/c-p chandrasekhar/changing-patterns-of-domestic-work/article22985402.ece
- Chen, M. A. (2011). Recognizing domestic workers, regulating domestic work: Conceptual, measurement, and regulatory challenges. Canadian Journal of Women and the Law, 23(1), 167-184.
- Chigateri, S., Zaidi, M., & Ghosh, A. (2016). Work Like Any Other, Work Like No Other103. Retrieved July 18, 2021, from http://www.unrisd.org/indiareport-chapter4
- Chigateri, S. (2021). Labour Law Reforms and Women’s Work in India: Assessing the New Labour Codes From a Gender Lens. Institute of Social Studies Trust.
- Indu, A., Indrani, M., & Neetha, N. (2012). Gender and migration: Negotiating rights, a women’s movement perspective. Delhi: Centre for Women’s Development Studies.
- International Labour Organisation (ILO). (2013a). Who are domestic workers? Ilo.Org. https://www.ilo.org/global/docs/WCMS_209773/lang–en/index.htm
- International Labour Organisation (ILO). (2013b). Global and Regional Estimates on Domestic Workers.
- International Labour Organisation (ILO), (2015). Indispensable yet unprotected: Working conditions of Indian domestic workers at home and abroad. Retrieved July 19, 2021, from https://www.ilo.org/wcmsp5/groups/public/—ed_norm/—declaration/documents/publication/wcms_378058.pdf
- Klemm, B., Däubler, W., Beimin, W., Lai, A., Min, H., & Sinha, S. (2011). Protection for Domestic Workers: Challenges and Prospects. Briefing Paper Special Issue, May, Friedrich Ebert Stiftung.
- Madhav, R. (2010). Legal Recognition of Domestic Work. Labour File, 8, 41.
- Mahanta, U., & Gupta, I. (2015). Road ahead for domestic workers in India: legal and policy challenges.
- Mazumdar, I., Neetha, N., & Agnihotri, I. (2013). Migration and gender in India. Economic and Political Weekly, 54-64.
- National policy for domestic workers. (2019, February 13). Retrieved July 18, 2021, from https://pib.gov.in/Pressreleaseshare.aspx?PRID=1564261
- Neetha, N. (2004). Making of female breadwinners: Migration and social networking of women domestics in Delhi. Economic and Political Weekly, 1681-1688.
- Neetha, N., & Palriwala, R. (2011). The absence of state law: Domestic workers in India. Canadian Journal of Women and the Law, 23(1), 97-120.
- Neetha N., & Indrani, M. (2020, June 01). Crossroads and Boundaries : Labour Migration, Trafficking and Gender. Retrieved July 19, 2021, from https://www.epw.in/journal/2020/20/review-womens-studies/crossroads-and-boundaries.html
- Overview of Labour Law Reforms (n.d.) Retrieved from https://prsindia.org/billtrack/overview-of-labour-law-reforms#_edn2
- Poddar, M., & Koshy, A. (2019). Legislating for Domestic’Care’Workers in India-An Alternative Understanding. NUJS L. Rev., 12, 67
- Shanthi, K. (2006). Female labour migration in India: Insights from NSSO data(Vol. 4, p. 2006). Chennai: Madras School of Economics.
- Sharma, S., & Kunduri, E. (2015). Of Law, Language, and Labour: Situating the Need for Legislation in Domestic Work. Economic and Political Weekly, 50(28).
- Singh, N., Keshri, K., & Bhagat, R. B. (2015). Gender dimensions of migration in urban India. In India Migration Report 2015(pp. 200-214). Routledge India.
- Srivastava, P., & Shukla, P. (2021). Crisis behind closed doors domestic workers’ struggles during the pandemic and beyond. Economic and Political Weekly, 17-21.
- Sumalatha, B. S., Bhat, L. D., & Chitra, K. P. (2021). Impact of Covid-19 on Informal Sector: A Study of Women Domestic Workers in India. The Indian Economic Journal, 00194662211023845.
Image Credit: ucanews.com










![Proposing a Legal Framework for Distribution of the COVID-19 Vaccination [Part I]](https://admin.thepeninsula.org.in/wp-content/uploads/2021/01/COVAXIN.jpg)


